
- Case-Based Roundtable
- General Dermatology
- Eczema
- Chronic Hand Eczema
- Alopecia
- Aesthetics
- Vitiligo
- COVID-19
- Actinic Keratosis
- Precision Medicine and Biologics
- Rare Disease
- Wound Care
- Rosacea
- Psoriasis
- Psoriatic Arthritis
- Atopic Dermatitis
- Melasma
- NP and PA
- Skin Cancer
- Hidradenitis Suppurativa
- Drug Watch
- Pigmentary Disorders
- Acne
- Pediatric Dermatology
- Practice Management
- Prurigo Nodularis
- Buy-and-Bill
Publication
Article
Dermatology Times
Rare tumors and fibrotic skin lesions
Author(s):
In this review article, Kaivon Sobhani, B.S., and, Eve Lowenstein, M.D., Ph.D., examine fibrotic skin lesions, including the cutaneous tumor dermatofibrosarcoma protuberan (DFSP).
Case Presentation
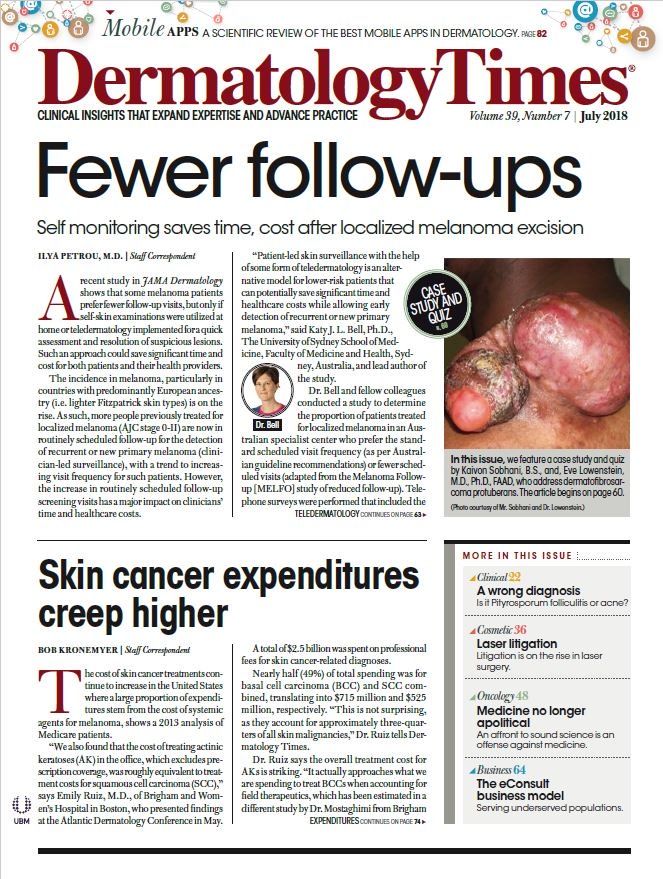
A 34-year-old African American male presents with a history of a painful lump on his left shoulder. He reports no trauma to the area. He noticed that the lump bled three days before. In addition, he noticed occasional paresthesias to his left hand, but denies fevers, chills, sweats, and weight loss. Physical examination of the left shoulder revealed an 8 x 4 x 3 cm ulcerative, nodular mass which was firm and mobile. The mass was nontender on palpation and showed no pus or active bleeding. The lesion was focally red and warm. In addition, the patient showed full strength and sensation in both upper extremities.
DISCUSSION
Dermatofibrosarcoma Protuberans (DFSP)
Dermatofibrosarcoma protuberans (DFSP) is an uncommon, cutaneous tumor characterized by aggressive local growth and a tendency to recur after surgical excision. DFSP typically presents as an asymptomatic, indurated plaque or firm cutaneous nodule in early adulthood.
The plaque can be red/brown, flesh colored, or blue/red and often is described with a previous history of trauma to the site. On palpation, the lesion is firm and is most commonly located on the trunk (60%), followed by the proximal extremities (30%) and head and neck (10%).1 Clinically, DFSP lesions may be mistaken for keloids, dermatofibroma and dermatomyofibroma.
The fact that the tumor is usually slow growing and asymptomatic often results in it being ignored by patient and physician and therefore treatment is frequently delayed. As DFSP slowly enlarges it may develop protuberant nodules. Once these nodules appear, growth can rapidly accelerate and the tumor can ulcerate and bleed, as in the case of the first patient.2 Even when DFSP become large, it is still uncommon for them to become fixed to underlying structures.3 How-ever recurrent DFSP may invade fascia, striated muscle, and bone. 4
DFSP is a tumor that arises in the dermis and shows the characteristic appearance of large spindle-shaped cells in a storiform pattern, which is a proliferation of fibroblastic tumor cells arranged around a central “hub” that resembles the spokes of a cartwheel.5,6 This finding has been shown to be histologically unique to DFSP.2 The condition can occasionally be confused histologically with other neoplasms such as fibrosarcoma, malignant fibrous histiocytoma, atypical fibroxanthoma, and dermatofibroma. Fibrosarcomas are composed of highly pleomorphic cells arranged in a herringbone pattern, which aides in differentiating them from DFSP.
Dermatofibromas
Dermatofibromas show overlying epidermal hyperplasia, small size, and occasional presence of many multinucleated giant cells.1 Immunoperoxidase staining has also proven to be a very useful tool in differentiating between these tumors. Dermatofibromas usually stain negative for CD34 but positive for factor XIIIa, while DFSP stain positive for CD34 and negative for factor XIIIa.7 Nearly all cases of DFSP have a gene mutation leading to the fusion of the collagen type 1a1 gene with the platelet-derived growth factor B-chain – a 17;22 translocation.8
DFSP accounts for less than 0.1% of all malignancies.3 The local spread of the tumor and its high likelihood to cause local recurrence after resection are due to the tentacle-like projections of tumor cells that invade between normal collagen bundles.1 Although DFSP is a very aggressive local tumor, it rarely metastasizes or leads to death. A high mitotic rate may indicate a greater potential for metastasis than tumors with a low mitotic rate.1,4
Complete surgical excision, especially Moh’s micrographic surgery (MMS), is the standard treatment for DFSP.9 High local recurrence rates are attributed to the tentacle like tumor growth pattern. The advantage of MMS is that it allows the surgeon to examine the deep and lateral margins of all the tissue that has been removed and therefore permit the detection of the tentacle-like projections of tumor while conserving the greatest amount of normal skin tissue. MMS offers highest cure rates for surgical excision of DFSP.1 Because the translocation (17;22) places the platelet derived growth factor (PDGF) β-chain gene under the control of the collagen 1A1 promoter, imatinib mesylate, which targets the PDGF receptor, has been tried in patients with DFSP. Currently, it is FDA-approved for adults with unresectable, recurrent, or metastatic DFSP.
Keloids and Hypertrophic Scars
DFSP may be mistaken clinically with a keloid, however keloids are benign growths with no metastatic potential and are the consequence to aberrant scar formation. Normal scars are flat and are preceded by injury. Hypertrophic scars are raised and confined to the site of injury. Unlike hypertrophic scars, keloids extend beyond the site of injury. They most commonly occur on the upper chest and arms, head and neck, and ear.10,11
Keloids have a smooth surface and are firm to hard to palpation. They may be pruritic or painful and can even inhibit normal motion of adjacent tissues. The keloids of this patient were so extensive that he had difficulty breathing. Patients often report a history of trauma at the site of keloid formation, for example an ear piercing, tattoo or vaccine injection. However, no reported trauma does not exclude a diagnosis of keloids. The above patient reported a history of a severe burn to his chest. Patients often also report a positive family history. Furthermore, black and Hispanic populations are more susceptible to keloids, with an incidence of 16% in black Africans.13 A number of genetic disorders, including Rubinstein-Taybi syndrome 1, Goeminne syndrome, Ehlers Danlos, and Turner syndrome, may predispose patients to developing keloids.14-16 Recently, keloids have been shown to have a higher incidence in Caucasian patients with the HLA-DRB1*1501 allele.17
Skin tension has been implicated as a factor in the formation of keloids, including post-surgical wound closure sites.18 Collagen synthesis is about 20 times greater in keloids than in normal, non-injured tissue. On histopathology, keloids exhibit thick hyalinized collagen bundles in a haphazard array with an increased number of fibroblasts. This is distinct from DFSP, which exhibits its characteristic storiform appearance. Generally, the overlying epidermis and papillary dermis are spared. In early keloids, there are abundant deposits of fibrillary collagen in the reticular dermis, however mature keloids often have thick, homogeneous, haphazardly arranged collagen bundles.
Immunohistochemical stains may also be performed to distinguish keloids and hypertrophic scars from DFSP. In contrast to DFSP, immunostaining for CD34 and Factor XIIIa is negative in keloids and hypertrophic scars.19,20
There is no universally accepted treatment protocol for keloids, although prevention continues to be the best strategy. Predisposed patients should avoid non-essential surgery. Treatment options typically include silicone elastomer sheeting, surgery with postoperative radiation therapy, and intradermal injections of intralesional steroids or chemotherapy.
See the related image IQ series and quiz: "When is a biopsy required?"
(All photos courtesy of Mr. Sobhani and Dr. Lowenstein)
Disclosures:
Kaivon Sobhani, B.S., is a medical student at SUNY Downstate Medical Center. Eve Lowen-stein, M.D., Ph.D., FAAD, is a dermatologist with the Health Science Center in Brooklyn and a dermatologist with South Nassau Dermatology PC in Oceanside and Long Beach, N.Y.
References:
1. Gloster HM. Dermatofi brosarcoma protuberans. J Am Acad Dermatol 1996;35:355-74.
2. Burkhardt BR, Soule EH, Winkelmann RK, et al. Dermatofibrosarcoma protuberans: study of fifty-six cases. Am J Surg 1966;111:638-44.
3. Bendix-Hansen K, Myhre-Jensen O, Kaae S. Dermatofibrosarcoma protuberans: a clinicopathological study of nineteen cases and review of world literature. Scand J Plast Reconstr Surg 1983;17:247-52.
4. McPeak CJ, Cruz T, Nicastri AD. Dermatofibrosarcoma protuberans: an analysis of 86 cases-five with metastasis. Ann Surg 1967;166:803-16.
5. Lever WF, Schaumberg-Lever G, editors. Histopathology of the skin. 7th ed. Philadelphia: JB Lippincott, 1990.
6. Taylor HB, Helwig EB. Dermatofi rosarcoma protuberans. A study of 115 cases. Cancer 1962;15:717-725.
7. Zelger B, Sidoroff A, Stanzl U, et al. Deep pentrating dermatofibroma vs. dermatofibrosarcoma protuberans: a clinicopathologic comparison. Am J Surg Path 1994;18:677-86.
8. Simon,M.P., Pedeutour,F., Sirvent,N., Grosgeorge,J., Minoletti,F., Coindre,J.M., Terrier-Lacombe,M.J., Mandahl,N., Craver,R.D., Blin,N. et al. 1997. Deregulation of the platelet-derived growth factor B-chain gene via fusion with collagen gene COL1A1 in dermatofibrosarcoma protuberans and giant -cell fibroblastoma. Nat.Genet. 15:95-98.
9. Gloster HM Jr, Harris KR, Roenigk RK: A comparison between Mohs micrographic surgery and wide surgical excision for the treatment of dermatofibrosarcoma protuberans. J Am Acad Dermatol. 35:82-87 1996 PMID: 8682970
10. Gilliet F, MacGee W, Stoian M, et. Al. Zur histogenese granuliertzelliger tumoren. Hautarza 1973; 2001;28:49.
11. Draaijers L, Templeman F, Botman Y, et al.: The patient and observer scar assessment scale: A reliable and feasible tool for scar evaluation. Plast Reconstr Surg. 113:1960-1965 2004 PMID:15253184
12. Van de Kar A, Corion L, Smeulders M, et al.: Reliable and feasible evaluation of linear scars by the Patient and Observer Scar Assessment Scale. Plast Reconstr Surg. 116:514-522 2005 PMID:16079683
13. Mentzel T, Wadden C, Fletcher CDM. Granular cell change in smooth muscle tumors of skin and soft tissue. Histopathology 1994;24:223.
14. Stevens CA, Pouncey J, Knowles D. Am. J Med Genet A. 2011 Jul; 155A(7):1680-4.
15. Goeminne L. A new probably X-linked inherited syndrome: congenital muscular torticollis, multiple keloids cryptorchidism and renal dysplasia. Acta Genet Med Gemellol (Roma) 1968; 17:439-67.
16. Lowenstein E.J., K. Kim and S. Glick, 2004. Dermatologic manifestations of Turner’s Syndrome. JAAD, 50: 767-776.
17. Brown JJ, Ollier WE, Thomson W et al. Positive association of HLA-DRB1*15 with keloid disease in Caucasians. Int J Immunogenet 2008; 35:303-7.
18. Nemeth AJ: Keloids and hypertrophic scars. J Dermatol Surg Oncol. 19:738-746 1993 PMID:8349914
19. Haycox CL, Odland PB, Olbricht SM, Piepkorn M: Immunohistochemical characterization of dermatofirosarcoma protuberans with practical applications for diagnosis and treatment. J Am Acad Dermatol. 37:438 1997 PMID:9308560
20. Kuo T, Hu S, Chan H: Keloidal dermatofi broma: report of 10 cases of a new variant. Am J Surg Pathol. 22:264 1998






")
")
")
")
")



















