
- Case-Based Roundtable
- General Dermatology
- Eczema
- Chronic Hand Eczema
- Alopecia
- Aesthetics
- Vitiligo
- COVID-19
- Actinic Keratosis
- Precision Medicine and Biologics
- Rare Disease
- Wound Care
- Rosacea
- Psoriasis
- Psoriatic Arthritis
- Atopic Dermatitis
- Melasma
- NP and PA
- Skin Cancer
- Hidradenitis Suppurativa
- Drug Watch
- Pigmentary Disorders
- Acne
- Pediatric Dermatology
- Practice Management
- Prurigo Nodularis
- Buy-and-Bill
Publication
Article
Dermatology Times
Is it acne or Pityrosporum folliculitis?
Author(s):
Review highlights the need to accurately diagnose this common bacterial infection.


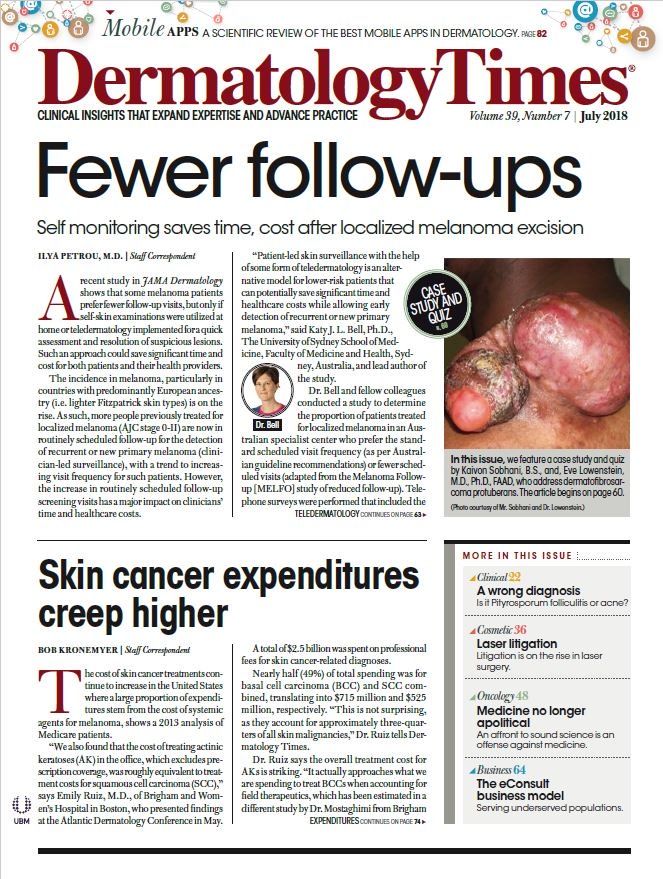
Pityrosporum folliculitis presents as fine monomorphic, pruritic papules and pustules appearing along the facial hairline and the upper back. It is sometimes treated with antibiotics, which can make the condition worse. (Photo courtesy of Brea Prindaville, M.D.)



Brea Prindaville, M.D.

Pityrosporum folliculitis is often mistaken by physicians as acne vulgaris, which can be a dire mistake leading to a worsening condition, shows a review published in the Journal of the American Academy of Dermatology.
“The reason it’s important to distinguish Pityrosporum folliculitis is that antibiotics used for acne actually make this worse. And azole antifungals make it better. So, the treatment is different,” says study author Brea Prindaville, M.D., a pediatric dermatologist and assistant professor, Warren Alpert Medical School of Brown University.
Acne and Pityrosporum folliculitis can occur together, given that acne patients often have increased sebum production and follicular hyperkeratinization resulting in occlusion, and acne is often treated with antibiotics. But while Pityrosporum folliculitis, which is caused by naturally-occurring yeast, appears similar in presentation to acne, there are important differences.
“Pityrosporum folliculitis usually presents as monomorphic keratosis pilaris-like fine papules and pustules. And it’s often pruritic. It’s often located on the upper forehead, extending into the hairline and the upper back,” Dr. Prindaville said.
Acne, on the other hand, isn’t usually pruritic. It typically presents as polymorphic lesions with open and closed comedones, inflammatory papules and pustules, as well as nodules and cysts, the authors write. Acne might appear in similar areas as Pityrosporum folliculitis, including on the forehead leading up to the hairline and occurring on the upper back.
WHAT THE REVIEW REVEALED
Dr. Prindaville and colleagues did a retrospective chart review of 110 Pityrosporum folliculitis patients (up to 21 years of age) who were seen in the dermatology department at the University of Massachusetts. More than 75 percent had acne that was treated with antibiotics and of those, 65 percent reported pruritus.
“Pityrosporum folliculitis was almost always described as numerous 1- to 2-mm monomorphic papules and pustules and often described as keratosis pilaris-like,” they write.
Fewer than one-fifth of patients studied had associated seborrheic dermatitis or tinea versicolor, although the authors write that the Malassezia yeasts that cause Pityrosporum folliculitis are also implicated in folliculitis, seborrheic dermatitis and tinea versicolor.
The forehead, often extending into the hairline, and upper back were the most common areas affected by Pityrosporum folliculitis.
While most of the patients in the study were white females, the authors note Pityrosporum folliculitis likely affects males and females, as well as all races similarly. Dr. Prindaville says the higher incidence of the skin condition among white females in this study could be due to a referral bias, rather than a true association.
“Females tend to be more bothered by their acne,” she says.
Pityrosporum folliculitis was more common after antibiotic use. More than 75 percent of the patients indicated they were treated with antibiotics for persistent acne, with more than half of those being prescribed oral antibiotics.
Only three of the Pityrosporum folliculitis patients studied had never had acne vulgaris, according to the authors.
And they found Pityrosporum folliculitis was quite common. Almost 5 percent of the 2,368 acne patient charts they reviewed indicated patients had Pityrosporum folliculitis at some point during their acne course, Dr. Prindaville said.
TREATING PITYROSPORUM FOLLICULITIS
Dr. Prindaville and her colleagues have had a good success treating Pityrosporum folliculitis with topical ketoconazole shampoo 2 percent, which is applied or 5-10 minutes every other day.
“Sometimes, if it’s severe, you need to combine that with oral [azole antifungal therapy]. But most people respond to the topical,” she says.
Three-quarters of the patients studied were treated with topical ketoconazole shampoo, which improved or resolved the condition for most. Patients with more severe disease benefited from either oral fluconazole and ketoconazole. Doctors prescribed from 100 mg daily for one week to 200 mg daily for three weeks of fluconazole. Dermatologists instructed patients to use ketoconazole 2 percent wash after oral therapy to prevent recurrence. In some cases, they used the wash alone at least until the follow up visit in two to three months.
About half of patients were free of Pityrosporum folliculitis within one to two follow-up visits. In fact, 100 percent of patients treated with each of these regimens improved: oral fluconazole, ketoconazole 2% shampoo used as a wash, ketoconazole 2% cream, ketoconazole 2% shampoo and cram or sulfur wash. But nine of the 12 patients treated with oral ketoconazole did not improve. The authors note oral ketoconazole hasn’t been an appropriate option for these patients since 2013, when the FDA strongly cautioned against using oral ketoconazole for superficial fungal infections because of risk of liver or adrenal injury.
While studies have suggested patients with Pityrosporum folliculitis need oral therapy, this paper shows that’s not necessarily the case, and most patients improve or clear with topical options.
REFERENCES
Prindaville B, Belazarian L, Levin NA, Wiss K. “Pityrosporum folliculitis: A retrospective review of 110 cases.” Journal of the American Academy of Dermatology. March 2018. DOI:10.1016/j.jaad.2017.11.022.






")
")
")
")
")















