
- Case-Based Roundtable
- General Dermatology
- Eczema
- Chronic Hand Eczema
- Alopecia
- Aesthetics
- Vitiligo
- COVID-19
- Actinic Keratosis
- Precision Medicine and Biologics
- Rare Disease
- Wound Care
- Rosacea
- Psoriasis
- Psoriatic Arthritis
- Atopic Dermatitis
- Melasma
- NP and PA
- Skin Cancer
- Hidradenitis Suppurativa
- Drug Watch
- Pigmentary Disorders
- Acne
- Pediatric Dermatology
- Practice Management
- Prurigo Nodularis
- Buy-and-Bill
Article
When flushing is more than embarrassment
Author(s):
Acute or irregular flushing may signal a more serious health condition, say researchers who list 14 questions physicians should ask patients complaining about unusual flushing.



(SaravootLeng-Iam/Shutterstock.com)
Once considered a harmless reaction to emotions, flushing is now known to be associated with more serious conditions in some cases.
“If a patient has an acute change, meaning they’ve never experienced flushing but now it’s occurring or occurring more frequently, plus, they have other symptoms - that’s a red flag. There are so many different types of cancers that can have flushing as a side effect which is why it’s important to screen patients and take a comprehensive review,” said Azeen Sadeghian, M.D., of Dermasurgery Center in Baton Rouge, La. Dr. Sadeghian is the author of two articles published in the September issue of Journal of the American Academy of Dermatology. One article focused on non-malignant causes of flushing and the second on malignant causes.
Dermatologists should be prepared to identify and investigate the cause of atypical flushing beginning with a full medical history, a review of symptoms, physical exam and laboratory and imaging tests, she said.
While most causes of flushing are benign, there causes that tend to be more insidious and sometimes, difficult to differentiate during presentation, Dr. Sadeghian said.
“It is not to say that a patient with hyperthyroidism or medication-induced flushing will not experience exacerbation of flushing responses to typical benign flushing stimuli. They can overlap. However, there are typically other notable aspects in their history that can help physicians differentiate between the two,” she says.
DEFINING SERIOUS
Defining what may be a serious problem associated with flushing can mean different things to different patients. Menopause-associated flushing can be embarrassing, but it’s not life-threatening. But there are cases in which flushing could signal an extensive list of neurologic issues.
“Usually neurologic forms of flushing are associated with other symptoms or they have a unique presentation. They can manifest on one half of the face, but not the other half. Or, they may appear on just a segment on the face,” Dr. Sadeghian said.
Medications can sometimes cause flushing, which can be problematic because it can lead to noncompliance.
While a life-long struggle with flushing might not bring a patient to the dermatologist’s office, new flushing, acute flushing changes or noticeably increased flushing might. These changes could be indicative of a more serious condition.
Life threatening conditions associated with flushing can include malignancy, serotonin syndrome, superior vena cava syndrome or other untreated systemic conditions. Red-flag symptoms include vague abdominal pain, diarrhea, back pain, random blood pressure spikes and severe headaches.
“Of these, we are the most cautious about catching an undiagnosed malignancy. For example, mastocytosis, thyroid cancer, bronchogenic cancer, pheochromocytomas, neuroendocrine tumors, renal cell carcinoma and others have been associated with flushing,” she says.
NEXT: Making the right diagnosis
THE RIGHT DIAGNOSIS


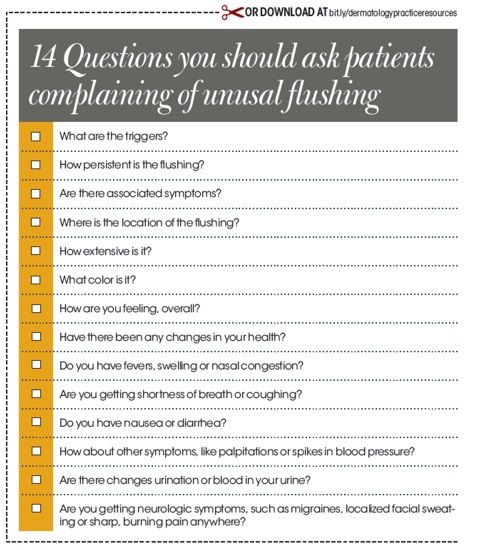
Simply asking about potential triggers can help tease out the cause of flushing. But people who have malignant causes can experience flushing from triggers, too. So, dermatologists may want to delve deeper, asking about how persistent the flushing is and the presence of associated symptoms. Other good questions include: Where is the location of the flushing? How extensive is it? What color is it?
“When patients experience skin changes, such as papules on the face, that’s when we think of rosacea. But if it’s isolated flushing, then you want to key into a complete review,” she says.
Follow-up questions include: How are you feeling, overall? Have there been any changes in your health?
Do you have fevers, swelling or nasal congestion? Are you getting shortness of breath or coughing? Do you have nausea or diarrhea? How about other symptoms, like palpitations or spikes in blood pressure? Are there changes urination or blood in your urine? Are you getting neurologic symptoms, such as migraines, localized facial sweating or sharp, burning pain anywhere?
“For example, if they’re getting muscle cramps, that might be a clue they have an electrolyte imbalance so it could be more than benign flushing,” she said. In this situation, Dr. Sadeghian recommends conducting a comprehensive review of systems and physical exam which will help delineate the direction of the laboratory workup which may include testing for 5-hydroxyindoleacetic acid (5-HIAA), histamine and tryptase levels, urine metanephrines, vanillylmandelic acid (VMA) and norepinephrine and vasoactive intestinal peptide.
Although many of lab testshaven’t changed in years, some institutions are evaluating the use of alternate markers. “For example, in medullary thyroid carcinoma, calcitonin is the usual initial serum screening test. Now we are seeing some groups advocate for procalcitonin, but the evidence still needs to accumulate before a dynamic shift in screening occurs. And although some laboratories have assays now to test for many of these tests, the patients’ samples may need to be processed differently than a lab system's default. In these situations, it would be best to contact the lab to ensure that proper processing is capable of being performed,” Dr. Sadeghian said.
Initial screening of these cancers may begin with basic laboratory assessments and possibly imaging. The patient should then be referred to an appropriate specialist for an in depth work up, diagnosis and staging, she said.
“We are beginning to see a dynamic shift in genetic testing for some of these cancers showing a potential heritable pattern. For example, in medullary thyroid carcinoma, DNA testing for the RET [rearranged during transfection] oncogene is now considered for family counseling purposes. This means family members can be tested and monitored appropriately,” Dr. Sadeghian said.
TREATMENT REMAINS A CHALLENGE
Flushing may always be difficult to manage, especially for those patients who do not appear to have an underlying cause.
“A lot of the medications that we use to treat it may not necessarily be a slam dunk. The best you can do is try to manage the underlying cause,” she said.
Dr. Sadeghian recommends educating patients about triggers and how to avoid them, as well as simple tips for when flushing occurs, such as applying a cold compress.
REFERENCES
Sadeghian A, Rouhana H, Oswald-Stumpf B, Boh E. “Etiologies and management of cutaneous flushing: Nonmalignant causes.” JAAD. September 2017. DOI: 10.1016/j.jaad.2016.12.031.
Sadeghian A, Rouhana H, Oswald-Stumpf B, Boh E. “Etiologies and management of cutaneous flushing: Malignant Causes.” JAAD. September 2017. DOI: 10.1016/j.jaad.2016.12.032.
Trimboli P, Seregni E, Treglia G, Alevizaki M, Giovanella L. “Procalcitonin for detecting medullary thyroid carcinoma: a systematic review.” Endocrine-Related Cancer. June 2015.










